-
Americas

-
Asia & Oceania

-
A-I
J-Z

EMEA Thought Leadership
Developing IQVIA’s positions on key trends in the pharma and life sciences industries, with a focus on EMEA.
Learn more -
Middle East & Africa

EMEA Thought Leadership
Developing IQVIA’s positions on key trends in the pharma and life sciences industries, with a focus on EMEA.
Learn more
Regions
-
Americas
-
Asia & Oceania
-
Europe
-
Middle East & Africa
-
Americas
-
Asia & Oceania
-

Europe
Europe
- Adriatic
- Belgium
- Bulgaria
- Czech Republic
- Deutschland
- España
- France
- Greece
- Hungary
- Ireland
- Israel
- Italia
EMEA Thought Leadership
Developing IQVIA’s positions on key trends in the pharma and life sciences industries, with a focus on EMEA.
Learn more -
Middle East & Africa
EMEA Thought Leadership
Developing IQVIA’s positions on key trends in the pharma and life sciences industries, with a focus on EMEA.
Learn more
SOLUTIONS
-
Primary Intelligence
-
Commercial Analytics
-
Management Consulting Services
-
R&D Solutions
-
Contract Sales and Medical Solutions
-
MedTech Solutions
-
Oncology Solutions
-
Real World Evidence Solutions
-
Technology Solutions
-
Supply Chain Solution
-
Provider Solutions
-
Public Health Solutions
Primary Intelligence
Today there is more data than ever. Each set of primary and secondary data provides important insights, but that data needs to be integrated. Current market research solutions leave a gap because they are unable to integrate the depth and breadth of insights required in today’s complex markets. IQVIA's Primary Intelligence is the exception.
Learn MorePrimary Intelligence Quick Links
Commercial Analytics
IQVIA provides segmentation and targeting, call planning and resource optimization, multichannel marketing, and performance management and compensation solutions for clients throughout the Middle East and Africa.
Learn MoreCommercial Analytics Quick Links
Management Consulting Services
IQVIA can help you take the decisions that lead to success. With a wide array of management consulting services and a patient-centric approach, we can help you succeed in today's healthcare market.
Learn MoreManagement Consulting Services Quick Links
R&D Solutions
IQVIA brings together human data, data science and human science to harness advances in technology, analytics and human ingenuity and enable a more modern approach to clinical development.
Learn MoreR&D Solutions Quick Links
Contract Sales and Medical Solutions
Healthcare is in a constant state of perpetual advancement and development, and healthcare businesses need to innovate and grow ahead of the market to succeed.
Learn MoreContract Sales and Medical Solutions Quick Links

MedTech Solutions
Today’s constantly developing technologies are pushing the boundaries of medical devices’ capabilities, adding new benefits and features that enhance patients’ lives and create new categories of buyers and influencers who play a larger role.
Learn More
Guiding through unprecedented innovations to reshape oncology
In the Middle East, oncology is increasingly becoming a major focus in healthcare. Today, it is the 6th highest selling therapy area and one of the fastest growing therapy areas in the region.
Learn More
You know your questions – let us bring you the right real-world answers
Your work promises the potential to improve health outcomes. At IQVIA, we strive to help you by providing you with the complete understanding, tools, evidence and communications you need to realize that potential. It’s an exciting time to reimagine what’s possible.
Learn MoreTechnology Solutions
With state-of-the-art technology and a global database, we help push the potential of human science higher and help our clients achieve it by improving healthcare professionals’ understanding of their patients’ needs.
Learn MoreTechnology Solutions Quick Links

Re-imagine pharmaceutical distribution and supply chain management
Digital disruption is empowering companies across industries with unbeatable competitive edge. Organizations that do not adopt and integrate digital technologies will experience debilitating disadvantages in a competitive marketplace.
Learn MoreProvider Solutions
IQVIA's comprehensive suite of healthcare provider solutions equip you with latest tools and technologies needed to build a smart and sustainable health setup. Talk to our experts and let us help you get started on your pathway to sustainable growth.
Learn MoreProvider Solutions Quick Links

IQVIA Public Health interventions work to improve the health of entire populations
IQVIA’s Public Health solutions offer powerful insights and innovative digital solutions with speed and agility to introduce modern approaches for public health surveillance and quality improvement.
Learn MorePRODUCTS
-
HCP Space
-
Hospital Information System
-
Mobile & Home Health
-
Revenue Cycle Management
-
Patient Level Information Costing System
-
IQVIA Health Insurance Management
-
IQVIA Vigilance Platform
-
SmartSolve eQMS: Enhance Quality Assurance and Control

HCP Space
Build deep HCP engagement journeys. Maximize digital engagement impact. Drive better brand outcomes.
Learn More
Hospital Information System
IQVIA’s cloud based solutions for healthcare providers and institutions are designed to minimize medical errors, increase physician efficiency, reduce costs, facilitate regulatory compliance and promote standardization of care to build a safer, more convenient way of managing healthcare.
Learn More
Mobile and Home Health Tech Solutions
IQVIA’s complete mobility suite for healthcare providers can help improve clinical teamwork, expand boundaries of care and drive better patient outcomes.
Learn More
Revenue Cycle Management
IQVIA can help you improve your billing and collection cycles, save processing time and help with better record keeping so that you can focus on providing the best patient care.
Learn More
Patient Level Information Costing System
IQVIA's PLICS, a patient costing solution, designed to help you better analyze your cost built using a bottom up Activity Based Costing methodology, developed by team of cost accountants specializing in Healthcare.
Learn More
IQVIA Health Insurance Management
An integrated platform that seamlessly connects patients, healthcare providers and payers to drive efficiency, reduce costs, and improve quality of care.
Learn more
IQVIA Vigilance Platform
Your complete, SaaS approach to drug safety and pharmacovigilance
Learn more
SmartSolve eQMS: Enhance Quality Assurance and Control
The complete eQMS for the Life Sciences industry.
Learn moreBLOGS, WHITE PAPERS & CASE STUDIES
Explore our library of resources spanning the healthcare ecosystem. Hear from IQVIA data scientists, doctors, researchers, and other experts on the topics, trends, and market developments that matter to you.
LEARN MORE
OUR LATEST WHITE PAPER
"Learn how digitalization has transformed the patient journey and why mapping the digital patient journey offers myriad of opportunities for pharma.
LEARN MOREABOUT IQVIA MIDDLE EAST & AFRICA
The IQVIA team in the Middle East and Africa works to provide clarity in these dynamic markets.
LEARN MORE
CAREERS
"Learn about work and life at IQVIA and find all the opportunities we have for your next step in your career journey.
Learn moreBlog
Are 'regional vaccine manufacturing hubs via PPP model' the answer to vaccine woes in Africa?
Sep 08, 2021
Africa manufactures only 1% of the 1.3 billion vaccine doses it administers annually.
Let that sink in.
Africa has the highest incidence of mortality caused by infectious diseases, but yet lacks the capacity to manufacture requisite vaccines. Africa depends on other countries for its vaccine needs – 99 percent of the continent's vaccines are imported. This dependence on imports leaves its citizens vulnerable to shortages of vaccines, causing health security challenges. The vaccine shortage indeed triggered a continent-wide crisis during the pandemic.
Vx Demand-Supply Dynamics – A Highly Concentrated Market
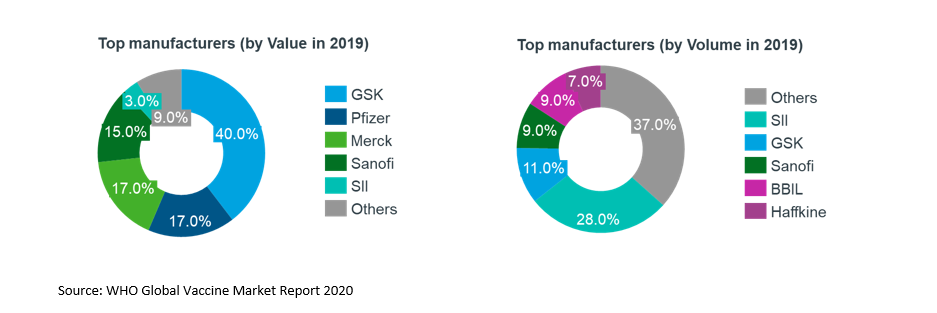
Global vaccine market size in 2019 was estimated to be 5.5B doses, which equates to approximately $33B in value. Global demand for vaccines is driven by governments of industrialized and developing countries, pooled procurement agencies, and private sector, with regulatory and advisory bodies overseeing vaccine quality.
Vaccine manufacturing is concentrated among large manufacturers such as GSK, Pfizer, Merck, Sanofi managing nearly 90% of the global value market. Only five manufacturers produce 60% of the global volume.
Large vaccine market share with only a few global manufacturers poses hindrance in key vaccine supply to low- and middle-income countries (LMICs). This has been particularly evident during the COVID crisis. Many early developers of COVID-19 vaccines entered into advance purchase agreements with rich nations, selling most of their Vx supplies to United States and Europe. As a result, countries in Africa, South America, and Asia have had a much lower vaccine coverage thus far and this trend is expected to continue. According to the World Health Organization (WHO), just a little more than 1 percent of the African population has been fully vaccinated against the COVID-19. Compare it to the U.S., where more than 50% of the population is already fully vaccinated.
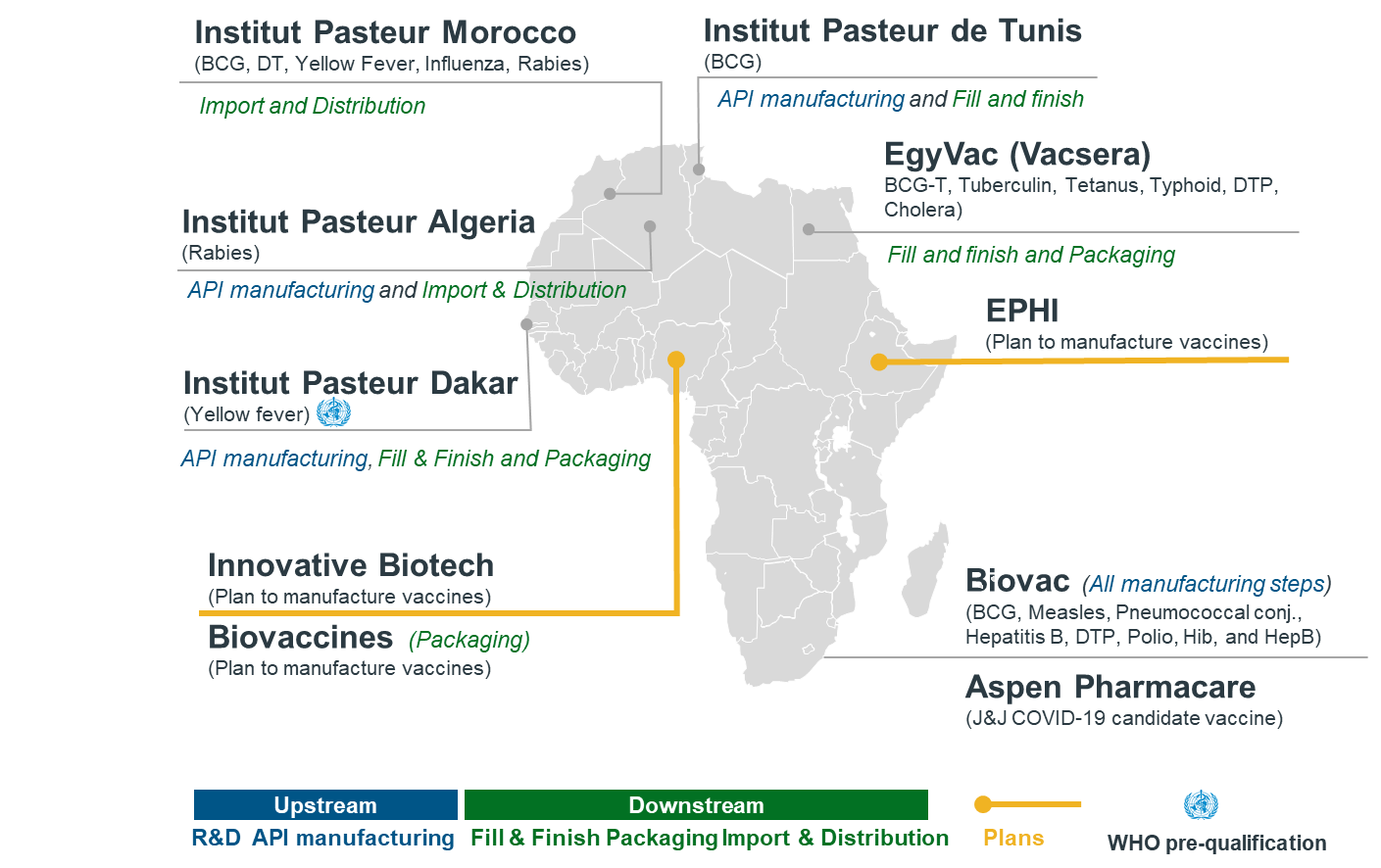
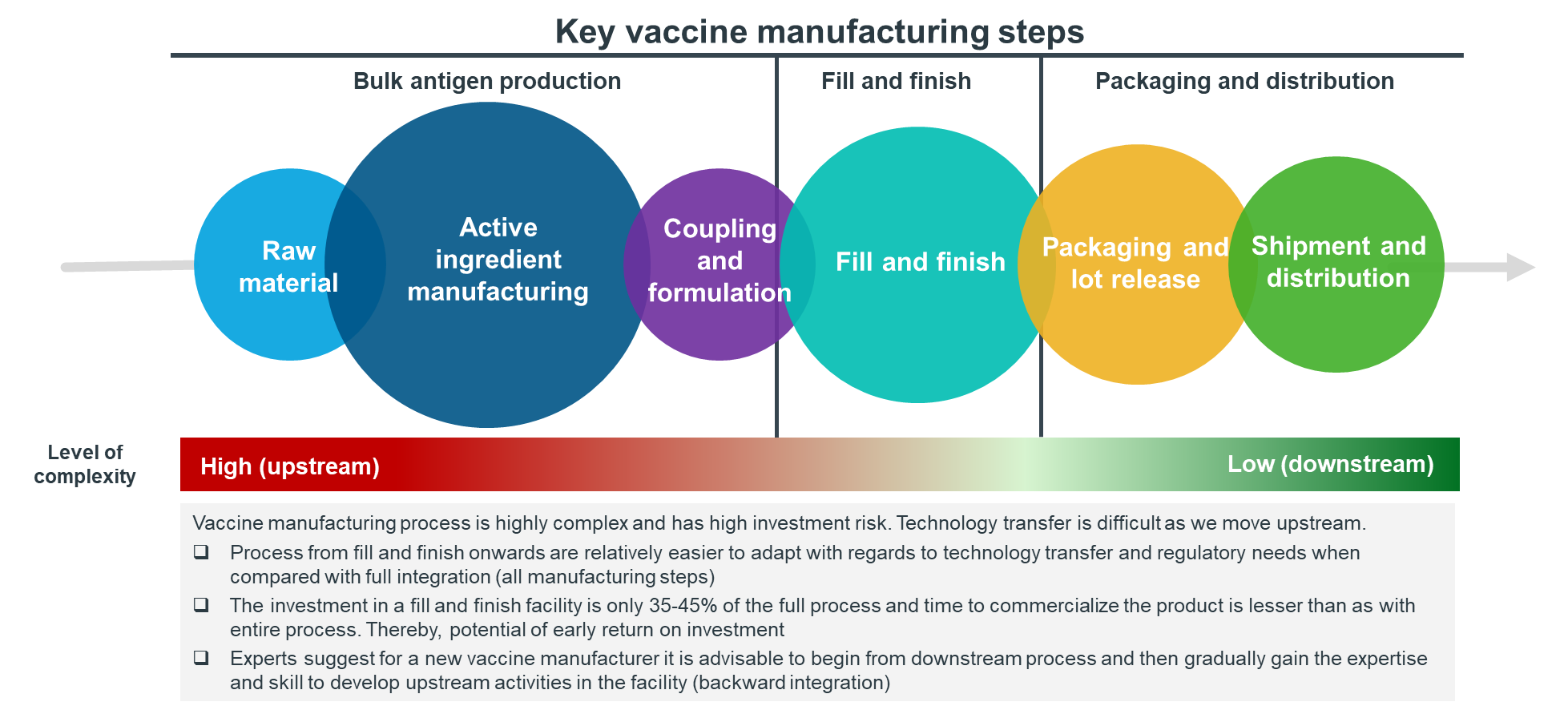
A Long Road Ahead to Build Vaccine Manufacturing Capabilities
Africa has a long way to catch-up, and the only way it can sustainably achieve vaccine security is by investing in building local vaccine manufacturing capabilities. Currently, there are only a few vaccine manufacturers in Africa, primarily executing downstream Vx manufacturing activities. As shown in the graphic below, most are more focused on fill and finish, while very few can manufacture vaccines from end-to-end.
Paving Way for a Bold Vision
By 2040, the African Union and the Africa Centers for Disease Control and Prevention aim to have 60 percent of routine vaccines consumed on the continent to be produced locally. Multiple initiatives are being undertaken towards this vision, including but not limited to:
- Influx of Funds from Key Players – IFC, along with four other institutions, will provide up to $14 million in grant funding to IPD (Senegal) along with project development support, helping it kickstart a manufacturing hub for COVID-19 and other vaccines.
- Support Offered by the Government – King Mohamed VI of Morocco officially announced the signature of 3 conventions with a) Sinopharm; b) Recipharm; and c) Sothema, for the construction of a new vaccine manufacturing facility in Morocco. The top priority will be given to the anti-COVID vaccine; however, future opportunities exist for building a smaller plant for other profitable vaccines.
- Collaboration with Global Manufacturers – Biovac (SA) will manufacture COVID-19 vaccines for Africa in collaboration with Pfizer and BioNTech. Biovac will acquire drug substance from Pfizer/BioNTech in Europe and perform fill/finish in South Africa. This showcases the capabilities, and tech transfer comfort with Pfizer, that Biovac has been able to build while working on the PCV13 vaccines over the years, enabling it to participate in the global vaccine supply chain for multiple products over time.
IQVIA point of view
The vision is definitely achievable, but Africa needs a change of strategy. We observe that various countries in Africa are adopting a rather fragmented and siloed approach around vaccine manufacturing, instead of a common, unified continent-wide strategy. The continent needs a long-term pan-African strategy, and not country-specific initiatives. Africa CDC and the African Union would benefit a lot more by promoting regional vaccine manufacturing hubs on the continent through public-private partnerships to achieve economies of scale and have feasible business models.
Distilling it at a more granular level, it means that for African countries looking to build local vaccine manufacturing, IQVIA has the following recommendations:- Focus on the high-value, expanding NIP routine vaccines such as Rotavirus and PCV, as it will be difficult to compete with existing DCVMs for legacy routine vaccines.
- Follow backward integration strategy, i.e., start with downstream vaccine manufacturing activities, build capabilities, and incrementally move upstream.
- Build regulatory capabilities and work towards WHO pre-qualification to supply through UNICEF/GAVI channels.
- Leverage urgent global action for anti-COVID vaccine manufacturing to develop public-private partnerships and capacity that can eventually extend to other vaccines.
- Establish partnerships with global manufacturers, facilitated by multilaterals through tech transfer hubs and incentivized by government through demand guarantees.
IQVIA has a dedicated public-health focused practice actively engaged with governments, national/international donors, non-governmental organizations (NGOs) and private sector stakeholders to support evidence-based decision making. Our service offerings include Policy and Strategic Planning, Disease Burden Assessment, Research and Analytics including undertaking large community and institutional surveys, Monitoring and Evaluations of Large programs, Procurement and Supply Chain Assessments, Digital Health in Public Health, Public-Private-Partnerships, Support Private sector engagement and Program Implementation. The public health team serves more than 20 countries in the Middle East, South Asia and African region. For more information, please reach out to Rishabh Jhol at rishabh.jhol@iqvia.com or Deepak Batra at DBatra@in.imshealth.com