-
Americas

-
Asia & Oceania

-
A-I
J-Z

EMEA Thought Leadership
Developing IQVIA’s positions on key trends in the pharma and life sciences industries, with a focus on EMEA.
Learn more -
Middle East & Africa

EMEA Thought Leadership
Developing IQVIA’s positions on key trends in the pharma and life sciences industries, with a focus on EMEA.
Learn more
Regions
-
Americas
-
Asia & Oceania
-
Europe
-
Middle East & Africa
-
Americas
-
Asia & Oceania
-

Europe
Europe
- Adriatic
- Belgium
- Bulgaria
- Czech Republic
- Deutschland
- España
- France
- Greece
- Hungary
- Ireland
- Israel
- Italia
EMEA Thought Leadership
Developing IQVIA’s positions on key trends in the pharma and life sciences industries, with a focus on EMEA.
Learn more -
Middle East & Africa
EMEA Thought Leadership
Developing IQVIA’s positions on key trends in the pharma and life sciences industries, with a focus on EMEA.
Learn more
SOLUTIONS
-
Research & Development
-
Real World Evidence
-
Commercialization
-
Safety & Regulatory Compliance
-
Technologies
LIFE SCIENCE SEGMENTS
HEALTHCARE SEGMENTS
- Information Partner Services
- Financial Institutions
- Global Health
- Government
- Patient Associations
- Payers
- Providers
THERAPEUTIC AREAS
- Cardiovascular
- Cell and Gene Therapy
- Central Nervous System
- GI & Hepatology
- Infectious Diseases and Vaccines
- Oncology & Hematology
- Pediatrics
- Rare Diseases
- View All

Impacting People's Lives
"We strive to help improve outcomes and create a healthier, more sustainable world for people everywhere.
LEARN MORE
Harness the power to transform clinical development
Reimagine clinical development by intelligently connecting data, technology, and analytics to optimize your trials. The result? Faster decision making and reduced risk so you can deliver life-changing therapies faster.
Research & Development OverviewResearch & Development Quick Links

Real World Evidence. Real Confidence. Real Results.
Generate and disseminate evidence that answers crucial clinical, regulatory and commercial questions, enabling you to drive smarter decisions and meet your stakeholder needs with confidence.
REAL WORLD EVIDENCE OVERVIEWReal World Evidence Quick Links

See markets more clearly. Opportunities more often.
Elevate commercial models with precision and speed using AI-driven analytics and technology that illuminate hidden insights in data.
COMMERCIALIZATION OVERVIEWCommercialization Quick Links

Service driven. Tech-enabled. Integrated compliance.
Orchestrate your success across the complete compliance lifecycle with best-in-class services and solutions for safety, regulatory, quality and medical information.
COMPLIANCE OVERVIEWSafety & Regulatory Compliance Quick Links

Intelligence that transforms life sciences end-to-end.
When your destination is a healthier world, making intelligent connections between data, technology, and services is your roadmap.
TECHNOLOGIES OVERVIEWTechnology Quick Links
CLINICAL PRODUCTS
COMMERCIAL PRODUCTS
COMPLIANCE, SAFETY, REG PRODUCTS

BLOGS, WHITE PAPERS & CASE STUDIES
Explore our library of insights, thought leadership, and the latest topics & trends in healthcare.
DISCOVER INSIGHTSTHE IQVIA INSTITUTE
An in-depth exploration of the global healthcare ecosystem with timely research, insightful analysis, and scientific expertise.
SEE LATEST REPORTS



FEATURED INNOVATIONS
-
IQVIA Connected Intelligence™
-
IQVIA Healthcare-grade AI®
-
IQVIA AI Assistant
-
Human Data Science Cloud
-
IQVIA Innovation Hub
-
Decentralized Trials
-
Patient Experience Solutions with Apple devices
WHO WE ARE
- Our Story
- Our Impact
- Commitment to Global Health
- Code of Conduct
- Sustainability
- Privacy
- Executive Team
NEWS & RESOURCES


Unlock your potential to drive healthcare forward
By making intelligent connections between your needs, our capabilities, and the healthcare ecosystem, we can help you be more agile, accelerate results, and improve patient outcomes.
LEARN MORE
IQVIA AI is Healthcare-grade AI
Building on a rich history of developing AI for healthcare, IQVIA AI connects the right data, technology, and expertise to address the unique needs of healthcare. It's what we call Healthcare-grade AI.
LEARN MORE
Meet the IQVIA AI Assistant
Your new expert analyst is here. Be at the forefront of data-driven decision-making with a new generative AI tool that enables you to interact with our products and solutions like never before. Get results you can trust, faster.
LEARN MORE
Your healthcare data deserves more than just a cloud.
The IQVIA Human Data Science Cloud is our unique capability designed to enable healthcare-grade analytics, tools, and data management solutions to deliver fit-for-purpose global data at scale.
LEARN MORE
Innovations make an impact when bold ideas meet powerful partnerships
The IQVIA Innovation Hub connects start-ups with the extensive IQVIA network of assets, resources, clients, and partners. Together, we can help lead the future of healthcare with the extensive IQVIA network of assets, resources, clients, and partners.
LEARN MORE
Proven, faster DCT solutions
IQVIA Decentralized Trials deliver purpose-built clinical services and technologies that engage the right patients wherever they are. Our hybrid and fully virtual solutions have been used more than any others.
LEARN MORE
IQVIA Patient Experience Solutions with Apple devices
Empowering patients to personalize their healthcare and connecting them to caregivers has the potential to change the care delivery paradigm.
LEARN MOREIQVIA Careers
Featured Careers
Stay Connected

WE'RE HIRING
"At IQVIA your potential has no limits. We thrive on bold ideas and fearless innovation. Join us in reimagining what’s possible.
VIEW ROLESBlog
Evolution of psoriasis endpoint use
Intensifying competition in the crowded psoriasis market drives trends in trial endpoints
Jul 31, 2020
Psoriasis Area and Severity index (PASI) is the most commonly used measure of skin disease in psoriasis patients. PASI measures the erythema, thickness, and scaling of psoriatic plaques and weights them by the size of the affected area to produce an absolute PASI score. Change in these absolute PASI scores, comparing before and after therapy, are the most commonly used psoriasis clinical trial efficacy endpoints. In these trials the endpoints are defined as the proportion of patients who achieve PASI 50, PASI 75, PASI 90, or PASI 100 which represent 50%, 75%, 90%, and 100% improvement in PASI score respectively. PASI 100 therefore equates to total plaque resolution and fully cleared skin, while lower numbers represent a lower degree of clearance.
As the available therapies treating psoriasis have become more efficacious over time, we could expect trials to use the highest PASI improvement thresholds as their endpoints. Trial designers are motivated to use the most stringent endpoint which the trialled drug could be expected to achieve as such designs provide the most compelling evidence supporting therapy use. This represents a pressure for companies to demonstrate the highest degree of efficacy for their drug, finely balanced against the risk of missing these endpoints.
Using data from the MARS database we have analysed the relative use of different PASI threshold endpoints from 2008-2019. The use of PASI 50/75/90/100 endpoints have been normalised to the number of all trials employing a PASI endpoint in a given year. The readout shown below (Fig. 1) demonstrates that there is an upward trend in the use of the more stringent PASI 90 and PASI 100 endpoints over the past ten years, whereas use of PASI 50 and PASI 75 has decreased.
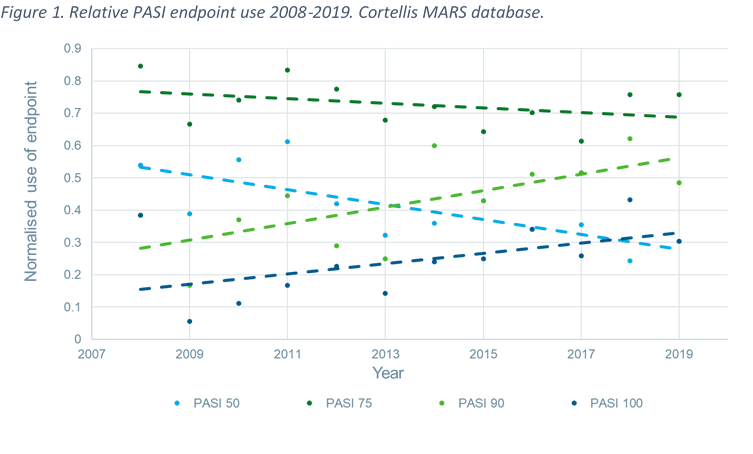
Use of the least stringent endpoint, PASI 50, can be shown to decrease most rapidly while PASI 75 use, although decreasing, is doing so at a slower rate and remains the most commonly used endpoint. Conversely PASI 90 use has increased rapidly and is approaching the level of PASI 75 use. Finally, PASI 100 use is increasing but remains the least used PASI endpoint, likely due to the difficulty in totally resolving skin plaques. PASI 100 use has however doubled over the past decade as newer biologics offer near curative action. Although PASI 100 is likely to become a required endpoint for trials, PASI 75 and PASI 90 could continue to be used as secondary endpoints. Therefore, although PASI 100 could become the new expected primary endpoint it may not overtake the use of other PASI endpoints according to analyses which use the same methodology as above.
These trends correlate with the introduction of more efficacious biologics and small molecules which have new mechanisms of action, such as anti-IL-17s, anti-IL-23s, and TYK-2 inhibitors. These newer drugs surpass the efficacy of older anti-TNFs, topical therapies, and non-targeted small molecules such as methotrexate.
Changes in psoriasis endpoint use add to a wider story in immunology markets of incremental innovation leading to market maturity, followed by a drive towards commercial and clinical differentiation for increasingly smaller patient populations.